

BRUNSWICK — P. Lynn Ouellette can’t help but laugh when she remembers the time her son tried to convince her that pumpkin bread should be a vegetable. He was so adamant, so persuasive, she almost agreed with him.
Growing up, Brendan Keating was a charmer, she recalled, smiling at the way her little boy would point and wink at strangers on the street or go over to the neighbors’ house for a visit before they were even awake. He was the kind of kid who took the motor out of his mom’s electric mixer because he had other plans for it.
And while she smiles when she thinks about her exuberant boy, who was somehow too big for every room, those memories are accompanied by waves of grief.
Keating died from an accidental heroin overdose five years ago, just a month shy of his 23rd birthday.
When he died in 2013, “he was an outlier,” Ouellette said. At the time, the opioid epidemic that would sweep across Maine and the rest of the United States was gaining traction. Five years later, law enforcement officials, doctors and others still are scrambling to rein in the epidemic and prevent more young lives from being lost.
Keating, a risk taker, struggled in school, suffering self-confidence problems with a high-achieving twin brother, an equally successful older sister and two physicians for parents. He was a good athlete but grappled with attention-deficit/hyperactivity disorder, and his grades weren’t good enough to keep him on the teams. When he graduated from high school, Ouellette was beside herself; excited, proud and relieved. After graduation, he enrolled at the Maine School of Masonry.
But it was clear when he was home that something was off. Keating was spending more and more time in his basement bedroom. He was irritable and didn’t sleep well.
Ouellette knew her son had experimented with marijuana as a teenager, and he had begun selling it when she turned him in to the police — something he never knew about — hoping to get him on the right track. When she discovered tin foil with burn marks in the basement, she knew Keating was using a more dangerous drug.
“He had a lot of denial,” she said. “He had anxiety and depression, but he kept a good mask.”
Even while he was stealing to support his habit, he and his mother had a good relationship. When Keating finally admitted to using opiates, Ouellette helped him get into the methadone clinic. He got clean, she said, but he relapsed after he started tapering his dosage.
“It got very scary,” she said. “Everyone was worried about him.”
Afraid she was going to get a call in the middle of the night, she told him she had proof he had stolen from her and forged checks, and that if he did not agree to go to a residential treatment facility, she would turn him in to the police.
“I told him, ‘I’m afraid you’re going to die and I’d rather have you in jail'” than dead, she said.
“Maine didn’t have a lot of options at the time,” before the opioid crisis hit the state with force, so he signed up for an eight-week program at an upscale facility in Arizona.
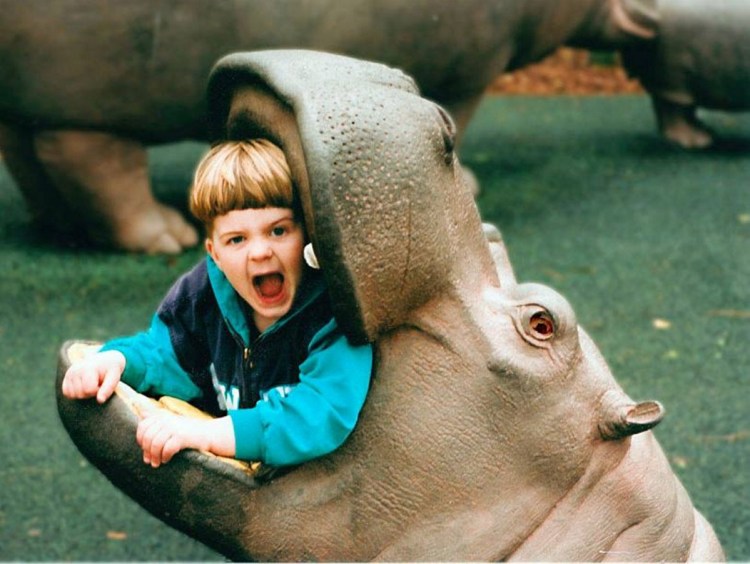
Lynn Ouellette holds one of the last photos her son Brendan took before his death in 2013 — his hands, caked in plaster, feeding a baby squirrel. Brendan struggled with self-esteem for much of his life; but even when things were bad, he and his mother had a good relationship, she said.
When Ouellette and her daughter, Katie, flew out to visit him for a family week, he begged them to let him come home, even though doctors had said he was not ready to leave.
Instead, Ouellette convinced him to enroll in a three-month program in California. There, they saw a shift. Keating was doing better, he was fully engaged in his recovery and he came home healthy. But life back home was not what Keating hoped it would be. He tried to get access to treatment nearby but didn’t stick with it. He had lost his driver’s license when he was in treatment, which he hadn’t known until he got back, making it hard to secure a job.
Before long, Ouellette could tell Keating was starting to slide backward, spending more time in the basement, getting irritable and defensive. She begged him to go back to the California facility.
“I could see the process starting again, but he would not acknowledge it.”
Then, one night in December 2013, the family found Keating unconscious in his room. He did not respond to Narcan, a drug used to treat opioid overdoses. He was rushed to the hospital, but by then his brain had been too long without oxygen. His sister, Katie, and twin brother Ryan came home to say their goodbyes, and on Dec. 16 the family turned off Keating’s life support.
Ouellette’s grief, her family’s grief, is ongoing.
“It’s a pain you don’t recover from,” she said, but her pain started years before, when Keating first started using. “There was fear all the time,” she said.
“You get a lot of tough love advice,” Ouellette added. “And you do have to be tough, but don’t leave out the love, and don’t give up on them. … I hung in until the end. I was a fierce mother.”
Watching the people pour in at her son’s wake, reading the letters and the cards people sent, seeing the donations sent into the scholarship they established in his name, Ouellette couldn’t help but think, “If only he could have seen this.”
FIVE YEARS ON
Keating’s story, while tragic, is not uncommon. In 2017, Maine reported 418 overdose deaths, with 109 of those in Cumberland County, 10 of them in Brunswick, according to police. While local numbers are thought to have decreased in 2018, statewide numbers have held steady — the first time in seven or eight years that the rates have not increased, according to Thomas Kivler, senior director of the Mid Coast Hospital Addiction Resource Center in Brunswick.
Lynn Ouellette, seated in her office, looks at a photo her son taken shortly before he died of an accidental overdose in 2013. “It’s a pain you don’t recover from,” she said of his death.
“We are living in a state where more than one person every day dies from an opioid overdose,” Kivler said. These people are young like Keating, they are older, wealthy and homeless. They have lives, families, jobs.”
Kivler and his team cannot save everyone, but with a model that has kept overdose deaths in Brunswick far below those of surrounding communities, they are doing the best they can.
“There is a specific reason and story for every single person that comes here,” he said, but everyone who does “has realized that their relationships with substances has gotten out of control.”
The Addiction Resource Center launched its own program for opioid use disorder in 2007 after realizing that the current program, which could take 11 days for a patient to be admitted to, “was just not OK.” When they brought the average down to under four days, it increased the clinics’ volumes by more than 500 percent, drawing people from as far away as Old Town who were desperate to get treated as soon as possible.
“At that time we were like the only game in town,” Kivler said.
It has since leveled off, and of the roughly 800 individuals the clinic sees per year, only 15 percent of the cases they take are for opioid use disorder, down from 35 percent when they first launched.
Aside from rapid admission, the Addiction Resource Center focuses primarily on intensive outpatient services, which they do at the clinic four days a week, three hours per day.
“For whatever reason, when people go away to a 28-day detox program, they don’t do as well when they come back,” Kivler said, citing a “bubble phenomenon” that occurs when people are completely surrounded by recovery services and then go back to their old lives with their old triggers everywhere.
Another key factor in the clinic’s success rate is its use of medication-assisted treatment with Suboxone, a prescription opiate-like medication that does not activate the opiate receptor the same way as heroin or other drugs, and can relieve symptoms of opiate withdrawal without the high or the danger of overdose. The use of Suboxone as treatment is on the rise since it does not have to be administered daily, unlike methadone. A recent report from the Maine Health Data Organization found that Suboxone is now the second-most-prescribed drug in the state, following a blood pressure medication and preceding an inhaler for asthma.
“The best science we have tells us that this is a chronic disease such as diabetes, such as asthma, and that’s how we treat it,” Kivler said, with medication.
Using a model developed at Yale, doctors will offer Suboxone to patients at the emergency room to help stop the withdrawal immediately, with the understanding that they will go on the next business day to the Addiction Resource Center, where they will administer the next dose and continue their treatment. This is the only such program in the state, Kivler said, although he does not think it will stay that way for long.
Admittedly, not as many people as he would like have taken them up on the offer, simply because they often are not ready to start the recovery process. For many people dealing with opioid addiction, the fear of withdrawal goes beyond any logical thought processes.
WITHDRAWAL ‘DEVASTATING’
Lynn Ouellette, seated in her office, looks at a photo her son taken shortly before he died of an accidental overdose in 2013. “It’s a pain you don’t recover from,” she said of his death.
Opioids are a class of drugs that include the illegal drug heroin, synthetic opioids such as fentanyl, which is more than 50 times more powerful than heroin, and pain relievers available legally by prescription, such as oxycodone (OxyContin), hydrocodone (Vicodin), codeine, morphine and many others, according to the National Institute on Drug Abuse. Addiction can start a number of ways, from intentional drug use to using prescription medication after an injury.
Keating suffered debilitating migraines as a child and was prescribed opioids to manage the pain at age 10, Ouellette said. She knows he did not abuse them as a child, but he was exposed to them.
The drugs are so powerful, in fact, that doctors at the addiction resource center warn patients that if they are going to relapse, to go back to one-third of their last dose, because once the body is not used to the drugs, a little bit can kill very quickly.
The brain has endogenous opioids, but when a drug is added to the mix, a massive bolus of dopamine is released, Kivler explained, resulting in a high. However, the brain self-regulates, and when that drug, is removed it lowers the hedonic set point, which is essentially how happy a person usually is. From extremely high dopamine levels to the new, lower-than-before levels once it wears off, the brain has to grapple to find a new mid-point, meaning that more drugs have to be used to get the same high.
Before long, people are using opioids just to function, Kivler said.
“Addiction lives in the brain stem, and people really believe they need their drug as much as they need to breathe or eat,” Kivler said. Someone in recovery once explained to him that craving a drug is like having someone hold your head underwater for 90 seconds and needing to breathe.
That’s when people start stealing from loved ones and doing things they would never do. “People will start to do desperate things because the brain thinks it’s a matter of survival,” Kivler said.
Leah Bauer, the behavioral health outpatient unit chief, said she is convinced the addiction “turns people into people they aren’t.”
“We don’t ‘believe’ that this is a medical condition,” Kivler said. “It is.”
Not only are the drugs incredibly powerful, but the withdrawal process, while perhaps not as “medically scary” as alcohol withdrawal, which causes seizures, is “physically and psychologically devastating,” Kivler said.
The feeling has been described as 100 times the worst flu imaginable, with “secretions coming from all the places you can secrete. Pain in the limbs and the heart and the muscles, joint. … It’s excruciating,” Kivler said. Aside from trying to function, many users keep using just to keep from getting sick, something Ouellette said Keating told her not long before he died.
“My son was tortured,” Ouellette said of the physical and emotional toll it took on him.
A LIFELONG FIGHT
Linda Pepin never considered herself a drug addict until the day she walked into Bridgton Hospital and sought recovery.
Linda Pepin “never intended to become a drug addict,” but after an abusive childhood, poverty and pain, she started down the path she never wanted to be on. Now, thanks to doctors and the medication Suboxone, she has been clean for two years.
Doing drugs was never much of a conscious decision for Pepin, 38. It was just something that happened after a lifetime of being around it. Growing up, “coffee brandy was like chocolate milk and wine coolers were like Kool-Aid,” she said.
When her brother was born, Pepin, only 7, was often left alone with the baby for days at a time; she had to resort to stealing just to feed her brother and herself. As she got older, she progressed to selling drugs to make more money, put more food on the table. By 20, she was using heroin and taking pills herself.
Her now-husband, Ray, helped get her away from an abusive home life and a stepfather who just a few years later was convicted of murdering her mother. But shortly afterward, Ray suffered injuries from an accident and was prescribed Oxycontin by his doctor.
“We made a killing” selling that for a while, she said, but seeing her husband turn into “a walking, talking mess (who) didn’t know his own name” when he was using scared her. She called his doctor and got him into a methadone clinic, fighting to keep him clean and hide her own addiction.
The two moved in 2008 to South Carolina to help care for Ray’s dying mother. He found another recovery clinic down there, but Pepin began to slip further away, taking some of her mother-in-law’s medication for herself. It wasn’t until Ray’s mother died, she said, that she finally “fell and broke.”
“She was the only real mother I had ever had,” she said. After that she started using crack, stealing money from her employer both in South Carolina and then again when they moved to Otisfield, Maine, and stealing from stores to support her addiction. She lost her license and racked up a $1,300 fine for it, drinking and using to cope with loss and with arthritis pain, which has been a daily struggle for more than half her life.
Pepin’s biggest fear always has been being the mother her mother was. Looking back, she is wracked with shame thinking of the things she did with her children in the car, thankful only that she did not hit rock bottom until after they were out of the house. She looks back at her worst years and is convinced that drugs and alcohol make you less than human. “It’s amazing what people will do when they’re not human,” she said. “I can’t imagine stealing now or being that dishonest.”
“I never intended to become a drug addict,” she said. “I fought my whole life to get my loved ones away from drugs and alcohol, and before I knew it, I was overtaken by it.”
It was Pepin’s niece who finally helped get her into recovery, introducing her to Dr. Peter Leighton, a primary care physician through Bridgton Hospital whose practice concentrates on medically assisted treatment for patients addicted to opiates. Like Kivler and Bauer, but in central Maine, Leighton is committed to helping treat his patients with humanity even when they feel they have lost their own. He also treats them with suboxone. Thanks to medication-assisted treatment, Pepin has been clean for two years, managing her arthritis with medication for restless leg syndrome and medical marijuana, but no other drugs.
After her husband’s experience with doctors and a recovery system that she says has destroyed him, she swore she would never see a doctor again. But Leighton, she said, “looks at you instead of the computer,” and he understands that recovery can only be successful if your well-being is balanced too. She sees Leighton once a month for suboxone and goes to counseling every two weeks.
The suboxone is what really has kept her clean, she said. It keeps her from feeling as though she really needs the drugs and allows her to regain some of the control over her brain. Unlike Methadone, about which she has “nothing good” to say, she does not need it every day, giving her some freedom.
Counseling has been another part of recovery that, like suboxone, she could not have made it so far without.
“I’ve needed the support,” she said. “It’s hard to see (the signs) that you’re falling, especially when you’re ready to give up. It’s important to have that outside help.”
She has friends, too, also in recovery, on whom she can lean if she needs support. And she does often; Pepin is now her husband’s primary caregiver because he suffers from cirrhosis of the liver, acute pancreatitis, diabetes, high blood pressure and a bad heart.
“You’re never fully recovered,” she said, but “I’m not going to let (the drugs) win. It just pushes me further.”
She is aware that relapse is possible and that for many, recovery is not a straight line. But she has been going strong for two years, and “in life I’ve always fought through everything. … I just don’t see relapse as an option.”
FIGHT FOR NARCAN ACCESS
Kivler, Bauer, Leighton and others have made strides in providing access to treatment in the Midcoast and beyond, but there is still work to be done to increase access, improve recovery systems, mitigate stigma and expand the availability of life-saving drugs such as the nasal spray naloxone, also known as Narcan.
Lynn Ouellette, seated in her office, looks at a photo her son taken shortly before he died of an accidental overdose in 2013. “It’s a pain you don’t recover from,” she said of his death.
The Addiction Resource Center will “make exceptions left and right,” Kivler said, and will “take everyone, regardless of their ability to pay.” However, the addiction resource cannot treat everyone in the area, let alone the entire state of Maine. Bauer said that lack of health insurance is a huge barrier for many addicts seeking treatment, and Ouellette believes that if Maine is going to beat this problem, “we need to expand Medicaid so people can get access to treatment.”
For those who do get themselves into treatment, recovery networks also need to be expanded. The Addiction Resource Network focuses on outpatient treatment in part because there is not the same kind of community established in Narcotics Anonymous as there is in Alcoholics Anonymous.
Relapses for opioid addiction are far too common, and according to Bauer, there are no opioid sober/recovery houses in the area. For people without a support network, surrounded by their former triggers, it can be hard to stay on the path of recovery.
“There are some people who just need more than what’s available” here, she said.
Ouellette and Bauer both are hopeful that what is available will change now that Gov. Janet Mills has taken office.
Former Gov. Paul LePage famously voted against legislation that would expand the availability of the opioid overdose-reversing drug Narcan. Mills, however, said during her campaign that she aimed to make Narcan “available to every family and agency that need it.”
“History will note that we have abandoned an entire generation of people to this preventable disease,” she said in her inaugural address. “It is time for action — Narcan widely available, medication-assisted treatment, recovery coaches. These things will be a reality.”
Mills went on to say that her administration will see the advent of a director of opiate response — “a person who will marshal the collective power and resources of state government to stem the tide of this epidemic.”
Narcan has saved more than 500 lives in Maine over the last two years alone. A recent study from Stanford estimated that increased availability to Narcan could prevent 21,000 deaths in the United States over the next decade.
“There’s more (Narcan access) now than there was five years ago, but we’ve had to fight for it because of political resistance,” Ouellette said. She does not think that Narcan would have saved Keating on the night of his overdose, but if she could go back, she would keep it in her house. It could have helped other times, she thinks.
The Brunswick Police Department has carried Narcan since June, with each officer equipped with two doses at a time. It was used only twice in 2018. Officer Jerod Verrill, Brunswick’s resident Maine Drug Enforcement Agency agent, is glad the officers are carrying Narcan now, following the lead of departments such as the Sagadahoc County Sheriff’s Office and Richmond Police Department. It is an opportunity to save lives and help get people back on track, he said, but he also has noticed that users are starting to carry Narcan. “There’s a theory that users can now push the limits,” he said.
To Bauer, that doesn’t matter.
“We can’t help people if they’re dead,” she said. “People will become ready for treatment on their own terms. Maybe that’s after one overdose or after 10 overdoses,” she said, but added that she will be there to help when they do.
There are other ideas about how to recover from a crisis that is killing thousands of Americans every year, such as stricter punishments for drug traffickers. Verrill said that last year, out of state drug traffickers accounted for a large quantity of illegal drug activity in the state.
“It seemed like as soon as we got one, they would send another one up,” he said.
In 2018 there were 66 drug arrests in Brunswick alone. The Brunswick Police Department also is digging more deeply into overdose death cases to try to determine who sold the drugs. This would lead to a “death resulting” charge and steeper consequences.
“We’re not going to be able to get rid of it completely, but we are doing the best we can to limit exposure,” he said.
Some communities also have seen positive outcomes from drug courts, something Bauer said she is interested in exploring further. Maine has six drugs courts — in York, Cumberland, Androscoggin, Penobscot, Hancock and Washington counties. Each serves 25 to 30 people who have pleaded guilty to nonviolent drug crimes. Participants work with health providers and a legal team to help keep them clean and away from further crime.
“Studies have demonstrated that accountability from the legal system can be very effective,” Bauer said, adding that she is eager to learn more about drug courts.
Perhaps one of the largest factors impeding recovery though, is the stigma against users, against their families.
“Addicts have so much shame. I watched it firsthand,” Ouellette said, noting how the concept of a “junkie” differs so drastically from the picture of her son, a young man raised in a family with two doctors.
“There’s the attitude that they deserve it because they got themselves into this process,” Bauer said, but it very quickly becomes not about seeking pleasure but avoiding pain. … Nobody wants to become a drug addict when they grow up.”
Pepin, too, hopes that sharing her story will help break the stigma and encourage others to come forward and seek treatment. “People are so embarrassed and ashamed,” she said. “The stigma that people choose this life … Who in their right mind would choose this?”
COPING WITH LOSS
Five years after her son’s death, and with so much left to be done to help make sure fewer parents experience the unbearable heartache she has gone through, Ouellette speaks openly and publicly about Keating’s struggles. As a physician, she has some clout, she said, to talk about it and to help reduce the stigma. Her son was not just a heroin addict.
He was a mason who built a stone walkway at her home that makes her want to stay there forever. He was a silly kid, a gifted athlete, a beloved brother and friend. After he died, a picture was found on his phone of his big hands, coated in plaster, feeding a baby squirrel. The photo now sits framed on her mantle. “That’s just who he was,” she said, looking at it.
His sister, Katie, volunteers her time at the needle exchange to try to connect with and help the person in front of her. But for Ouellette, it’s the public speaking that, while hard, feels like the best use of her energy.
“I so loved my son,” she said. “I want his life to count for something.”
Send questions/comments to the editors.
