

It was early April and things were not looking good in Maine. The state’s COVID-19 caseload had been doubling every four days. Hospitalizations were climbing. Arenas in Portland and Bangor were being prepared to serve as field hospitals in case those cities’ intensive care units were overwhelmed by the steadily increasing number of people acutely sick with the disease, as was already happening in New York.
Nobody was sure what would happen. Models suggested that by August, Maine could have as few as 100 deaths, or more than 1,000.
Then, around April 11, Dr. Dora Anne Mills, a former director of the Maine Center for Disease Control and Prevention, remembers breathing a sigh of relief as she examined the new case data: It had been flat for a week. “It was very emotional to see because I knew we could be in enormous trouble and it all depended on whether the state had shut down in time or not and we just didn’t know,” says Mills, chief health improvement officer at MaineHealth and the younger sister of Gov. Janet Mills. “I remember saying to people, ‘I think we’re going to be OK.’”
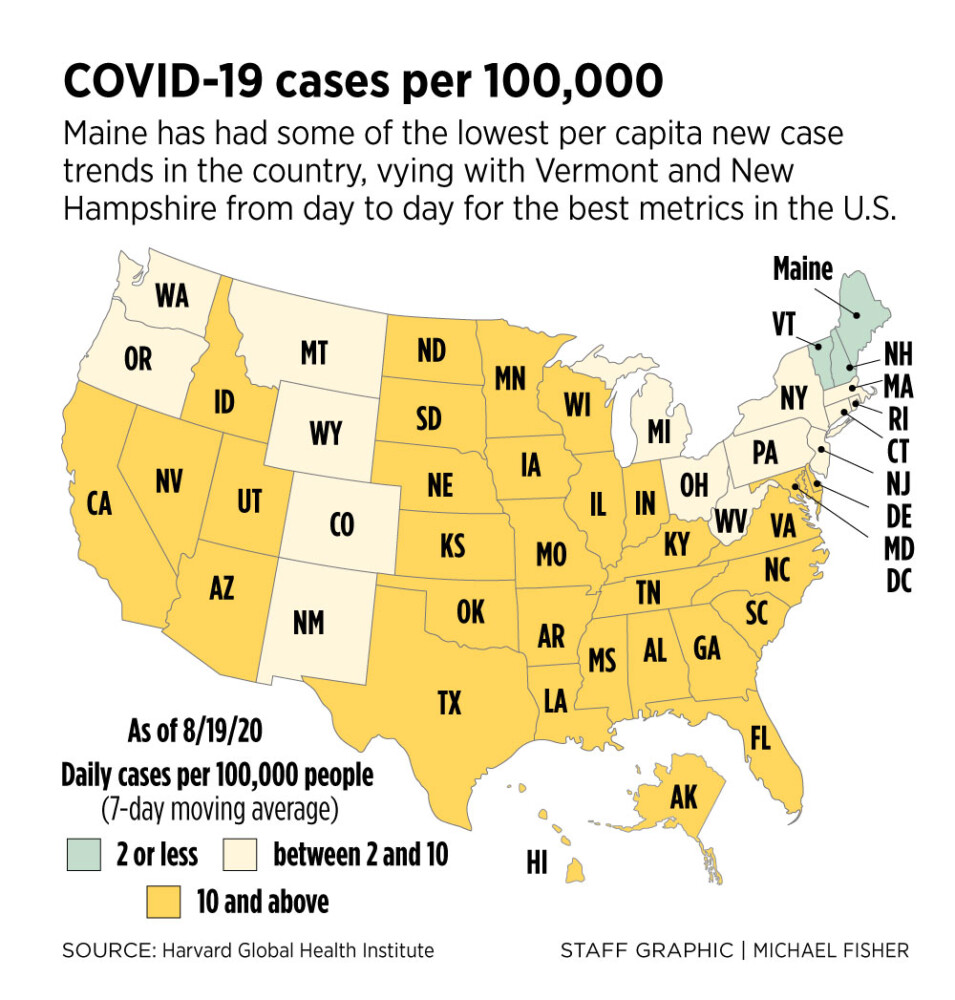
More than five months into the pandemic and nearing the end of the summer tourist season, Maine is doing more than OK. For weeks, the state has had among the lowest per capita new case trends in the country, vying with Vermont and New Hampshire from day to day for the best metrics in the country. Hospitalizations for the disease have for the past month been at the lowest levels since the first days of the pandemic. This past week, Maine’s per capita deaths from the disease – 1 per 100,000 residents – were the second lowest in the country after Vermont. The positivity rate for COVID-19 tests – which public health experts say should be under 3 – stood at under 0.8 percent.

A sign was posted near the south entrance of Maine Medical Center in Portland on April 2. Staff photo by Derek Davis
“Maine has consistently been doing very well and all of these indicators definitely seem incredibly encouraging,” says Divya Siddarth, a research fellow at Microsoft and co-author of a series of reports assessing states’ pandemic response organized by Harvard’s Edmond J. Safra Center for Ethics. “It’s not a fluke; something is working.”
How did Maine win the first rounds of its battle with COVID-19, containing the initial outbreak in March and then managing a phased reopening of its economy and tourism industry without the disease gaining a new foothold? Experts from across Maine and the nation say it appears to be a combination of early luck, fortuitous geography, good policy, and, ultimately, a prolonged commitment by Maine’s people to protect one another from the deadly, highly contagious disease that’s ravaged the world.
All of that could change at any time, as recent events in Millinocket have shown. Nearly half of the 65 people who attended an indoor wedding reception there on Aug. 7 tested positive for the disease, and at least 21 others have become infected in connection with it, including a woman who died Friday, illustrating how quickly the disease can take hold when social distancing guidance is ignored. But to date, Mainers have succeeded in curbing the disease to a remarkable degree compared to most of the rest of the country.

“I know people will say that so-and-so wasn’t wearing a mask and that so-and-so wasn’t taking it seriously, but Maine residents have done the right thing pretty consistently,” says Dr. Cheryl Liechty, an infectious disease physician and hospital epidemiologist at Pen Bay Medical Center in Rockport. “Now it’s a matter of making it really clear that we have to be in it for the long haul, because the schools are depending on us doing that.”
An Unfolding Storm
Since just after the turn of the new year, the pandemic had been gathering like a storm front on the horizon. A mysterious disease outbreak in the Chinese city of Wuhan led authorities to order the strict lockdown Jan. 23 of a region of 18 million people. By then, 13 were dead there and the first cases had already been confirmed in Thailand, South Korea, Japan and Washington state, suggesting a highly contagious disease was already spreading with airline passengers across the globe. Two weeks later, more than 900 were dead in China alone, and the infection was spreading through cruise ships. By March 8, northern Italy was under lockdown, with hospitals and morgues overwhelmed, and the army was soon deployed to process the dead.
The afternoon of Thursday, March 12, the pandemic got real in Maine. An Army reservist from in her 50s from the Lewiston-Auburn area who had just returned from northern Italy had come to Central Maine Medical Center’s emergency room after experiencing COVID-like symptoms. Her test – made possible by the arrival of the first testing ingredients in Maine just three days earlier – came back positive. The next day an employee of Portland’s India Street Public Health Center was sick with the disease, prompting 23 colleagues to go into quarantine. Schools across southern Maine closed for the day and Portland’s city manager canceled the first cruise ship calls and closed the doors of City Hall.

Gov. Janet Mills, center, gives updates about state efforts to test for and deal with the coronavirus on March 12 at the State House in Augusta. The governor announced Maine’s first positive test for the coronavirus. Staff photo by Joe Phelan Buy this Photo
On Sunday, March 15 – Maine’s 200th birthday – the confirmed case count had jumped to seven, including two residents of Falmouth’s Ocean View nursing home and a 12-year old student at Cape Elizabeth Middle School. Ambulance crews were under quarantine. Gov. Mills declared a state of emergency, recommending the voluntary closure of schools, the cancellation of non-emergency medical procedures and gatherings of more than 50. In southern Maine, many people effectively began locking down.
Forty-eight hours later the case count had jumped to 32 in seven counties, even though testing ingredients were in such short supply that only the most acutely symptomatic people were being tested. One was a child under the age of 10. Some bowling alleys, movie theaters, and microbreweries were still open. Gov. Mills ordered the mandatory closure of bars and restaurant dining rooms and a ban on gatherings of more than 10. A week later there were 142 confirmed cases and hospitals in Portland and Brunswick began filling with very sick patients. In New York City there were then over 18,000 confirmed cases and hundreds of dead and dying.
“We were on the surge curve, there was no doubt, but nobody knew the extent of the cases out there,” recalls Dora Anne Mills, who watched the doubling rate of cases with alarm. “With this virus, if you get far enough along the pandemic surge curve a shutdown isn’t able to control it – you can’t stop it – and that’s what happened in New York: exponential growth, like an explosion.”
As cases continued to rise, Gov. Mills ordered all nonessential public-facing business to close March 24 and, on March 31, issued a mandatory, statewide stay-at-home order. “These are no ordinary times,” she explained. “Extraordinary actions are required.” There were 303 confirmed cases and five Mainers had died.

The board room at Maine Medical Center filled with members of the Hospital Incident Command System (HICS) during their daily meeting on Thursday, March 12. Staff photo by Brianna Soukup
The first week of April, MaineHealth and Northern Light Health began preparations to create field hospitals at Cross Insurance Arena in Portland and Cross Insurance Center in Bangor in case Maine Med, Mercy, and Eastern Maine Medical Center were overwhelmed. The clinical leadership of all the state’s hospital networks – normally competitors – had been working together to coordinate responses, including contingency plans to move less acute patients to smaller hospitals to free up space at the major trauma centers.
“Even though we were prepared to use the field hospital concept if we needed to, that was the last resort in everybody’s mind,” recalls Dr. Joan Boomsma, MaineHealth’s chief medical officer. “There wouldn’t be the same ability for hygiene and plumbing and oxygen, but we realized there might be a need for patients who are less acute but might need to be quarantined.”
As the Maine CDC waited in vain for ventilators from the federal strategic stockpile, state-by-state models estimated a wide range of possibilities for Maine, depending on how well the disease had been contained. The University of Washington’s widely cited model predicted 115 deaths by August. The Johns Hopkins University one estimated 200 to 300 deaths if transmission were reduced by 70 percent, but more than 1,000 if the reduction was only 60 percent.
But Maine was lucky. By fortune and perhaps circumstance – with the Canadian borders closed and no scheduled international flights, we were relatively isolated – the disease wasn’t widespread in the community when the state started locking down March 15. Starting April 4 the new caseload began to flatten, rather than increase, at a level of around 25 to 35 a day, and would remain at those levels for the next three weeks. Hospitalizations peaked at the end of that week and began a gradual glide downward, relieving fears the state’s medical system would be overwhelmed.

Dr. Nirav D. Shah, director of the Maine Center for Disease Control and Prevention, talks to staff after a press conference about COVID-19 at the Maine Emergency Management Agency in Augusta on March 27. Staff photo by Derek Davis
“We took a hammer to the curve and as a result of the sacrifices made in March and April, our baseline prevalence of the disease was low enough so that when we started social and economic activity, the likelihood of a person encountering another person and having transmission occur was very low,” said Dr. Nirav Shah, director of the Maine CDC.
This was a good thing in that Maine CDC was impaired in tracking the progress of the disease, potentially courting disaster. It was unable to say how many COVID-19 patients were hospitalized on a given day – a key metric of the burden on hospitals – until April 10, and for months was the only state in the country unable to provide a basic daily pandemic tracking metric, the number of tests performed and the percentage of those that tested positive, which it finally began releasing June 3.
Reopening angst
With the state locked down and hospitals beginning to look safe, the Mills administration began studying how and when to safely begin reopening. Public health experts were advising governments not to reopen until they had robust testing and contact tracing regimes in place so any new flare-ups triggered by increased social contacts could be detected and isolated quickly.
Facing heavy pressure from business and industry, Mills announced April 28 that Maine would take its first steps toward reopening on May 1, when barbershops, hairdressers, auto dealers, doctor’s offices and golf courses would be allowed to reopen statewide. But at the time, Maine had not met key thresholds laid out by the White House and the U.S. Centers for Disease Control and Prevention in mid-April: a “downward trajectory” of cases for at least 14 days or, failing that, a reduction in the positive share of coronavirus tests compared to 14 days earlier. At the time, Maine’s new case trend had been ascending for nearly a week and the state was experiencing an increasing trend in the positivity rate of tests.
The state also didn’t have robust testing and contact tracing in place, though there were plans in the works. A partnership with Westbrook-based Idexx Laboratories announced May 7 nearly tripled the Maine CDC’s in-house testing capacity, but by mid-May – when most businesses in 12 counties had reopened – Maine’s testing rate was still below the bare minimum threshold of 1,805 tests a day recommended for the state by the Harvard Global Health Institute. (Daily testing wouldn’t begin regularly exceeding this threshold until late June.)

A sign at City Hall in Portland indicates it is closed to visitors April 1. Staff photo by Shawn Patrick Ouellette
Meanwhile, the disease began a resurgence almost immediately, propelled by outbreaks in fish processing plants and long-term care facilities and in immigrant neighborhoods in Lewiston-Auburn where many employees of the plants and nursing homes lived. Cumberland County saw a steep increase in cases in the first week of May, and by the third week in May much of southern Maine was back to peak pandemic case counts and hospitalizations. A single assisted living facility, Cape Memory Care in Cape Elizabeth, posted 57 new cases in a single day May 21, and MaineMed’s inpatient count matched the first surge peak of 35 on May 25.
On May 28, Gov. Mills postponed the reopening of restaurant dining rooms in Maine’s three southernmost counties, which had been slated for June 1, but allowed the reopening of most retail stores statewide.
“Despite negative feedback, the governor had the courage to back off on restaurants being open when the data indicated they should not be,” says Dr. Lani Graham, a former Maine CDC director.
And then this second surge began to recede, with most pandemic indicators ebbing through June, July, and early August, even as the economy reopened and tourists and summer visitors from states with higher disease prevalence returned. To the surprise of many experts, there has been no indication to date of any transfer of the disease from visitors to Mainers, and the state’s case counts, positivity rates, and hospitalization trends have generally remained at the lowest levels since the early days of the pandemic.
Improved testing, broad compliance save summer
Experts credit improved safety procedures and testing for greatly reducing the number of outbreaks in congregate settings. “There were pretty significant structural changes around that time: shelters for people experiencing homelessness; more Plexiglas in Maine businesses; having workers facing the same direction in seafood plants; symptom checks for employees,” says Dr. Shah. “These things in concert really helped our congregate settings.”

Dr. Hayley Weber, the director of molecular biology at NorDx Laboratories, far right, talks with employees in the lab on March 12. Staff photo by Brianna Soukup
“At the same time, we were really ramping up our testing a lot so we could catch the one case before it could turn to 10 or 50,” Shah adds. “The deal with Idexx really allowed us to liberalize our own rules with respect to testing and kept the one case to 50 case scenarios from happening.” This month, daily tests in Maine started regularly exceeding 2,500.
Dr. Thomas Tsai of the Harvard T.H. Chan School of Public Health says this investment in testing capacity has been critical to Maine’s success. “Maine has done a good job in terms of maintaining a high level of testing even with relatively low numbers of cases,” he says. “It’s now at a stage where Maine can recognize the embers before they turn into bonfires.”

Raymond Millette reads a newspaper in a bus stop shelter on April 7 near the Biddeford Police Department, where a sign advises people arriving from out of state to self-quarantine for 14 days. Staff photo by Gregory Rec
Public compliance with social distancing and masking guidelines has probably been the most critical factor in avoiding a summer resurgence of the disease, even as other parts of the country have experienced uncontrolled outbreaks. Last week, southern Maine businesses and law enforcement heads reported that compliance has greatly increased since May, with fewer customers objecting to wearing masks or following other rules.
“We certainly have enough people in enough communities who are doing enough to keep infection rates very low,” says Dr. John Alexander, chief medical officer for Central Maine Medical Center’s parent, Central Maine Healthcare in Lewiston. “But we’re not at zero yet.”
Tourists – who if from Massachusetts and 44 other states are subject to 14-day quarantine requirements – have appeared to take the measures seriously also, possibly because many of them are from places in the Northeast that suffered devastating outbreaks in March and April. “Maine has benefited from the good job its regional neighbors have done, which means out-of-staters coming to Maine are less likely to be bringing the disease with them,” says Jeremy Youde, who studies the intersection of government and public health at the University of Minnesota Duluth.
Visitors from higher-prevalence areas may also be more disease-conscious, says Dr. Peter Millard, an epidemiologist. “The tourists by and large have been more careful than the Mainers,” says Millard, a former U.S. CDC staffer who is now medical director at Seaport Community Health Care in Belfast. “There have been some cases, but they haven’t led to community spread, so that’s good news.”
Dr. Shah, whose leadership many sources cited for the successful response, also gives credit to the public for keeping the disease in check, and urged them not to let their guard down. “I think we’re in good shape, but things could change,” he says. “We are by no means immune from the upticks we are seeing in other states.”
Send questions/comments to the editors.
